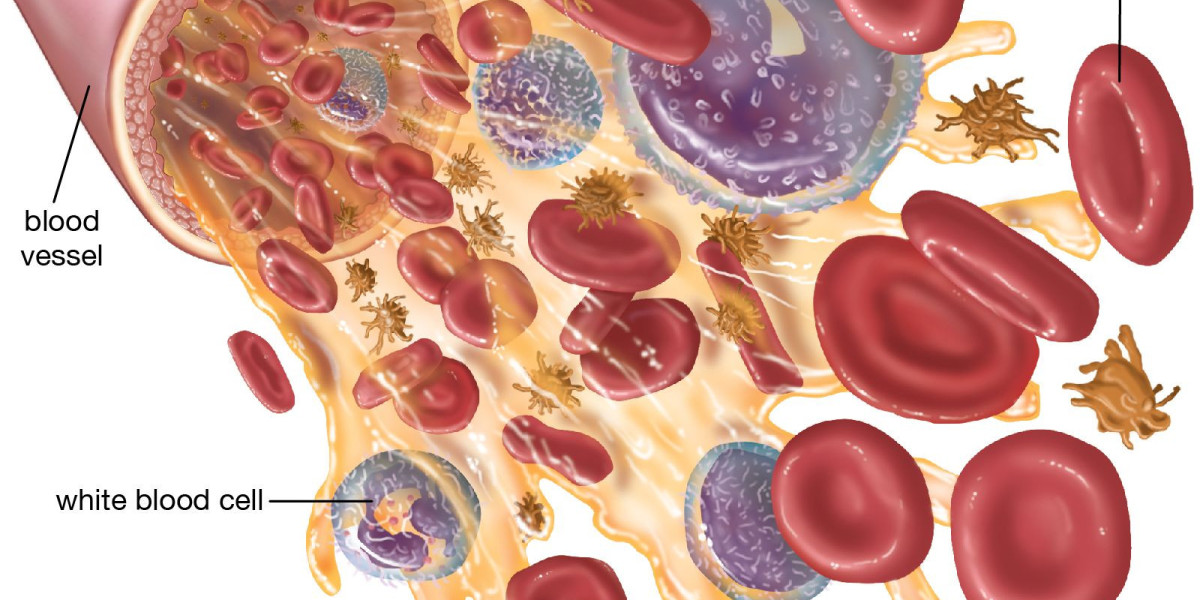
White blood cells (WBCs), or leukocytes, are integral components of the human immune system and serve as the body's principal defenders against infectious agents, foreign materials, and abnormal cells. They circulate through the bloodstream and lymphatic system, continuously monitoring for pathogens, toxins, and physiological anomalies.
Although they account for only a small fraction of total blood volume, their biological importance is disproportionate to their quantity. Understanding the various types of white blood cells and their associated functions is essential for clinicians, researchers, and healthcare supply chain professionals including those operating in pharmaceutical distribution channels such as a ceftriaxone injection wholesaler who must maintain a working knowledge of how immune mechanisms respond to bacterial, viral, and parasitic threats.
White blood cells can be broadly categorized into two primary groups: granulocytes and agranulocytes. These classifications derive from the presence or absence of granules in the cytoplasm when cells are examined under a microscope. Each subtype possesses a specialized functional portfolio that contributes to overall immunologic integrity.
Granulocytes
Neutrophils
Neutrophils are the most abundant type of WBC and represent the body’s first line of defense against bacterial invasion. They react rapidly to chemotactic signals released at infection sites and possess a formidable arsenal of antimicrobial mechanisms, including phagocytosis, degranulation, and production of reactive oxygen species. Neutrophils are short-lived cells, typically surviving only a few hours to days, but their swift mobilization is crucial to controlling acute infections. Elevated neutrophil counts often indicate bacterial infection, inflammation, or physiologic stress, whereas low levels may increase vulnerability to opportunistic pathogens.
Given the centrality of neutrophils in combating bacterial threats, antimicrobial agents such as ceftriaxone commonly distributed through a ceftriaxone injection wholesaler play an important role in clinical settings where neutrophil-mediated defense is insufficient. Understanding neutrophil activity helps inform therapeutic decision-making and supports effective antimicrobial stewardship.
Eosinophils
Eosinophils are primarily associated with host defense against parasitic infections and play a key role in allergic responses. These cells contain granules rich in cytotoxic proteins such as major basic protein and eosinophil peroxidase, which can damage parasites and modulate inflammatory processes. Eosinophils also contribute to tissue remodeling and immune regulation. Elevated eosinophil levels often occur in conditions such as asthma, allergic rhinitis, helminthic infections, and certain autoimmune disorders. Their regulatory activities underscore the complexity of immune responses beyond simple pathogen elimination.
Basophils
Basophils are the least common granulocytes but have a significant impact on immune signaling. They participate in hypersensitivity reactions, particularly those mediated by immunoglobulin E (IgE). Basophils release histamine, leukotrienes, and other inflammatory mediators when activated.
These substances increase vascular permeability and attract additional immune cells to sites of injury or infection. Basophils also contribute to defense against ectoparasites and play emerging roles in modulating adaptive immunity. Despite their low prevalence, dysregulated basophil activity can contribute to chronic inflammation and allergic disease.
Agranulocytes
Monocytes
Monocytes circulate in the bloodstream before differentiating into macrophages or dendritic cells upon entering tissues. These cells bridge the innate and adaptive branches of the immune system. Macrophages perform phagocytosis, secrete cytokines, process antigens, and orchestrate inflammatory responses. Dendritic cells serve as professional antigen-presenting cells (APCs), capturing antigens and presenting them to T lymphocytes to initiate adaptive immunity. Monocytes are also involved in tissue repair and homeostatic regulation. Their versatility makes them essential for clearing pathogens, controlling chronic inflammation, and maintaining immunologic balance.
Lymphocytes
Lymphocytes are central players in adaptive immunity and include three principal subtypes: T cells, B cells, and natural killer (NK) cells.
T cells regulate immune responses and carry out cell-mediated immunity. Subsets include helper T cells (CD4+), which coordinate immune signaling; cytotoxic T cells (CD8+), which destroy infected or abnormal cells; and regulatory T cells, which maintain immune tolerance and prevent excessive inflammation.
B cells are responsible for humoral immunity. Upon activation, they differentiate into plasma cells that secrete antibodies targeted to specific pathogens. These antibodies neutralize toxins, facilitate phagocytosis, and aid in complement activation.
NK cells function within the innate immune system but act independently of antigen sensitization. They recognize and eliminate virus-infected cells and malignancies through cytotoxic mechanisms.
Coordinated Immune Response
Although each white blood cell subtype has distinct responsibilities, the immune system is fundamentally cooperative. Granulocytes initiate rapid responses to infection, providing immediate protection. Agranulocytes subsequently build targeted, long-term defenses while ensuring immune regulation and memory formation. These integrated processes allow the body to control acute infections, prevent reinfection, and maintain vigilance against emerging threats.
When pathogens overcome initial defenses particularly drug-resistant bacteria therapeutic interventions become essential. This is one reason why the global supply chain for antimicrobials requires high operational reliability. Even stakeholders outside direct patient care, such as procurement units or a ceftriaxone injection wholesaler, must understand the clinical relevance of immune function to appreciate the critical nature of timely antimicrobial distribution.
Clinical Relevance of White Blood Cell Evaluation
Laboratory evaluation of WBCs is a cornerstone of diagnostic medicine. A complete blood count (CBC) with differential provides quantitative data on each leukocyte subtype. Deviations from reference ranges can indicate infection, systemic inflammation, hematologic malignancies, autoimmune disorders, and bone marrow dysfunction.
For example
Neutrophilia may indicate bacterial infection or physiologic stress.
Lymphocytosis may occur in viral infections or chronic inflammatory states.
Monocytosis can accompany chronic infections or autoimmune diseases.
Eosinophilia frequently suggests allergic reactions or parasitic exposure.
Basopenia or basophilia may reflect chronic inflammation or endocrine abnormalities.
Clinicians interpret these patterns in conjunction with patient symptoms, diagnostic imaging, and microbiological findings to develop an evidence-based treatment plan.
Conclusion
White blood cells orchestrate the body’s defense against a vast range of biological threats through a highly coordinated system of innate and adaptive responses. Each leukocyte subtype contributes specialized functions rapid microbial clearance, immune regulation, memory formation, and tissue surveillance that enable the immune system to operate with precision. An understanding of these mechanisms is essential not only for medical practitioners but also for organizations operating in pharmaceutical supply chains, including a ceftriaxone injection wholesaler, where awareness of immune processes supports informed decisions about antimicrobial demand, inventory strategy, and distribution priorities.
By appreciating how various white blood cells function and interact, stakeholders across the healthcare continuum can better support efforts to manage infection risk, maintain public health, and ensure the availability of critical therapeutic agents.















